| Cut It Out! | Risky business | That thing is going where? | Placenta... not to be confused with polenta |
|---|---|---|---|
|
What is cesarean hysterectomy
What is the first line treatment of placenta accreta?
|
What is 7-9%
Maternal mortality with placenta accreta has been reported to be as high as ___?
|
What is normal placentation?
|
What is a placenta with the leading edge <2.0 cm from the internal os.
A low-lying placenta is defined by?
|
|
What is 34 weeks
What does ACOG recommend as the ideal time for delivery of placenta accreta?
|
What is 3-5L
What is the average EBL at delivery with a woman with a pregnancy complicated by placenta accreta?
|
What is placenta previa?
|
What is 36 weeks and without amniocentesis.
A patient with placenta previa should be delivered at ___ weeks, ____(with/without) amniocentesis to assess for fetal lung maturity?
|
|
What is every 2-3 hours or every 1500 mL EBL
At what point during a cesarean hysterectomy should you redose prophylactic antibiotics?
|
What is a woman with prior myometrial damage secondary to cesarean section with either anterior or posterior previa overlying the prior scar.
What women are at greatest risk of placenta accreta?
|
What is placenta accreta?
|
What is a hypoechoic boundary between the placenta and the bladder.
On ultrasound, a normal placental attachment site is characterized by ___?
|
|
What is (1) epidural for uterine artery balloon and/or ureteral stents followed by (2) general anesthesia immediately prior to abdominal incision
What is the ideal anesthesia plan for planned cesarean hysterectomy?
|
What is 1 in 533.
What is the approximate incidence of placenta accreta?
|
What is placenta percreta?
|
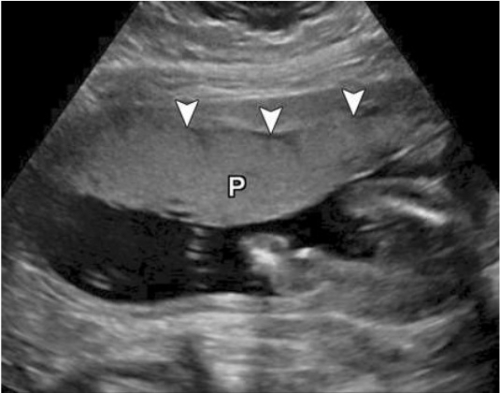
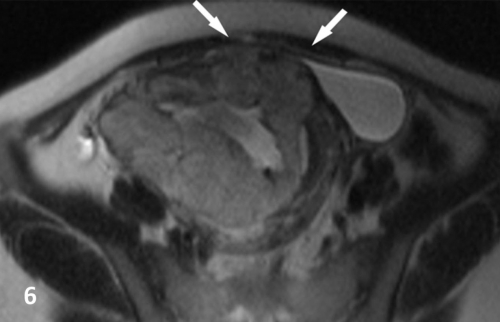
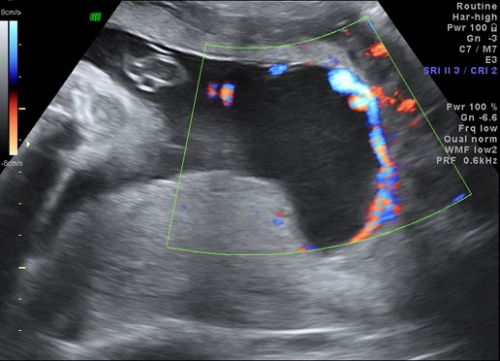
What is irregularly shaped placental lacunae ("moth-eaten" or "Swiss cheese" appearance), thinning of the myometrium overlying the placenta, loss of the retroplacental "clear" space," protrusion of the placenta into the bladder, increased vascularity of the uterine serosa-bladder interface, and turbulent blood flow through the lacunae on Doppler ultrasonography. FYI: the presence and increasing number of lacunae within the placenta at 15-20 weeks of gestation have been shown to be the most predictive ultrasonographic signs of an accreta, with a sensitivity of 79% and a PPV of 92%.
Name some signs of placenta accreta that can be noted on ultrasound (give 2)?
|
|
What is anesthesia, OB, gyn oncology, neonatology; consider urology and IR.
What clinical services should you consider consulting prior to planned cesarean hysterectomy? Give at least 4.
|
What is ~40%.
3/11/40/61/67% for 1st/2nd/3rd/4th/5th repeat cesareans.
A 24 y/o G4P3003 presents to your office at 20 weeks for her first prenatal visit. She has a history of 3 prior cesarean sections. You perform an anatomy ultrasound and note a placenta previa. You tell her she is at increased risk of having a placenta accreta compared to the average patient and may end up requiring a more extensive surgery depending on findings at the time of repeat cesarean section. What is her approximate risk of placenta aacreta with her history of 3 cesareans and placenta previa?
|
What is vasa previa?
Type I occurs when there is a velamentous cord insertion between the umbilical cord and placenta, and fetal vessels running freely within the amniotic membranes overlie the cervix or are in close proximity to it. Pregnancies with resolved placenta previa or low-lying placenta are at risk for Type I vasa previa. Type II occurs when the placenta contains a succenturiate lobe or is multilobed (typically bilobed), and fetal vessels connecting the 2 placental lobes course over or near the cervix. Although no standardized criteria exist regarding how close the fetal vessels must be to the internal os to constitute vasa previa, a threshold of 2 cm has been proposed. Delivery recommended between 34-37 weeks depending on patient stability. Antenatal hospitalization has been proposed for women with pregnancies complicated by vasa previa, beginning at 30 to 34 weeks’ gestation, and in one series, more than half of such individuals followed as outpatients subsequently required hospitalization for a complication. The purpose of hospitalization is to allow for closer surveillance for signs of labor and to perform cesarean delivery in a timely manner to avoid membrane rupture. Membrane rupture can lead to very rapid fetal exsanguination (SMFM guidelines) |
What is previous placenta previa (recurrence rate 4–8%), caesarean delivery, myomectomy or endometrium damage caused by D&C. Women who are younger than 20 are at higher risk and women older than 35 are at increasing risk as they get older
What are some risk factors for placenta previa (name 3)?
|
|
Placenta adherens.(placenta adherens is caused by failed contraction of the retroplacental myometrium)
What is the most common cause of retained placenta after a normal spontaneous vagina delivery?
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}